TA的每日心情 |
2018-10-15 10:59 |
|---|
|
今天读了Stockley's Drug Interactions 8th Edition,其中阿司匹林与ACEI的相互作用有详细的说明,供大家参考:
The antihypertensive efficacy of captopril and enalapril may be reduced by high-dose aspirin in about 50% of patients. Low-dose aspirin (less than or equal to 100 mg daily) appears to have little effect. It is unclear whether aspirin attenuates the benefits of ACE inhibitors in heart failure. The likelihood of an interaction may depend on disease state and its severity.
Renal failure has been reported in a patient taking captopril and aspirin.
Clinical evidence
A. Effects on blood pressure
(a) Captopril
Aspirin 600 mg every 6 hours for 5 doses did not significantly alter the blood pressure response to a single 25 to 100-mg dose of captopril in 8 patients with essential hypertension. However, the staglandin response to captopril was blocked in 4 of the 8, and in these patients, the blood pressure response to captopril was blunted.1 In another study, aspirin 75 mg daily did not alter the antihypertensive effects of captopril 25 mg twice daily in 15 patients with hypertension.
(b) Enalapril
Two groups of 26 patients, one with mild to moderate hypertension taking enalapril 20 mg twice daily and the other with severe primary hypertension taking enalapril 20 mg twice daily (with nifedipine 30 mg and atenolol 50 mg daily), were given test doses of aspirin 100 and 300 mg daily for 5 days. The 100-mg dose of aspirin did not alter the efficacy of the antihypertensive drugs, but the 300-mg dose reduced the antihypertensive efficacy in about half the patients in both groups. In these patients, the antihypertensive effects were diminished by 63% in those with mild to moderate hypertension and by 91% in those with severe hypertension. In contrast, another study in 7 patients with hypertension taking enalapril
(mean daily dose 12.9 mg) found that aspirin 81 mg or 325 mg daily for 2 weeks did not have any significant effect on blood pressure.4 A further study in 18 patients also found that aspirin 100 mg daily for 2 weeks did not alter the antihypertensive effect of enalapril 20 or 40 mg daily.
(c) Unspecified ACE inhibitors
In a randomised study, the use of low-dose aspirin 100 mg daily for 3 months did not alter blood pressure control in patients taking calciumchannel blockers or ACE inhibitors, when compared with placebo.
Similarly, in a re-analysis of data from the Hypertension Optimal Treatment (HOT) study, long-term low-dose aspirin 75 mg daily did not interfere with the blood pressure-lowering effects of the antihypertensive drugs studied, when compared with placebo. Of 18 790 treated hypertensive patients, about 82% received a calcium-channel blocker, usually felodipine alone or in combination, and 41% received an ACE inhibitor, usually in combination with felodipine.
B. Effects in coronary artery disease and heart failure
Various pharmacological studies have looked at the short-term effects of the combination of ACE inhibitors and aspirin on haemodynamic parameters. In one study in 40 patients with decompensated heart failure, aspirin 300 mg given on the first day and 100 mg daily thereafter antagonised the short-term haemodynamic effects of captopril 50 mg given every 8 hours for 4 days. The captopril-induced increase in cardiac index and the reduction in peripheral vascular resistance and pulmonary wedge pressure were all abolished.8 In another study, in 15 patients with chronic heart failure receiving treatment with ACE inhibitors (mainly enalapril 10 mg twice daily), aspirin in doses as low as 75 mg impaired vasodilatation induced by arachidonic acid.9 In yet another study, aspirin 325 mg daily worsened pulmonary diffusion capacity and made the ventilatory response to exercise less effective in patients taking enalapril 10 mg twice daily, but did not exert this effect in the absence of ACE inhibitors.10 However, results from studies are inconsistent. In a review,11 five of 7 studies reported aspirin did not alter the haemodynamic effects of ACE inhibitors whereas the remaining two did. In one of these studies showing an adverse interaction between aspirin and enalapril, ticlopidine did not interact with enalapril.
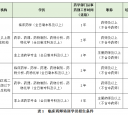
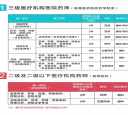
A number of large clinical studies of ACE inhibitors, mostly post-myocardial infarction, have been re-examined to see if there was a difference in outcome between those receiving aspirin at baseline, and those not. The results are summarised in ‘Table 2.2’, (p.15). However, in addition to the problems of retrospective analysis of non-randomised parameters, the studies vary in the initiation and duration of aspirin and ACE inhibitor treatment and the length of follow-up, the degree of heart failure or ischaemia, the prognosis of the patients, and the final end point (whether compared with placebo or with the benefits of aspirin or ACE inhibitors). The conclusions are therefore conflicting, and, although two meta-analyses of these studies found no interaction, an editorial13 disputes the findings of one of these analyses.14 In addition to these sub-group analyses, there have been a number of retrospective cohort studies. A retrospective study involving 576 patients with heart failure requiring hospitalisation, showed a trend towards an increased incidence of early readmissions (within 30 days after discharge) for heart failure among subjects treated with ACE inhibitors and aspirin, compared with those treated with ACE inhibitors without aspirin (16% versus 10%). In patients without coronary artery disease the increase in readmissions was statistically significant (23% versus 10%).15 However, long-term survival in heart failure was not affected by the use of aspirin with ACE inhibitors. Furthermore, among patients with coronary artery disease there was a trend towards improvement in mortality in patients treated with the combination, compared with ACE inhibitor without aspirin (40% versus 56%).16 Similarly, a lack of adverse interaction was found in a retrospective study involving 14 129 elderly patients who survived a hospitalisation for acute myocardial infarction. However, the added benefit of the combination over patients who received either aspirin or ACE inhibitors alone was not statistically significant.
Similarly, in another cohort of patients discharged after first hospitalisation for heart failure, there was no increase in mortality rates or readmission rates in those taking aspirin and ACE inhibitors.18 In another retrospective analysis in patients with stable left ventricular systolic dysfunction, no decrease in survival was seen in patients receiving ACE inhibitors, when comparing those also receiving aspirin (mean dose 183 mg daily, 74% 200 mg or less) and those not. Conversely, another study found that, compared to patients not taking aspirin, the use of high-dose aspirin (325 mg daily or more) with an ACE inhibitor was associated with a small but statistically significant 3% increase in the risk of death, Whereas low-dose aspirin (160 mg daily or less) was not.
C. Effects on renal function
Acute renal failure developed in a woman taking captopril when she started to take aspirin for arthritis. Renal function improved when both were stopped.21 However, in a re-analysis of data from the hypertension Optimal Treatment (HOT) study, long-term low-dose aspirin 75 mg daily had no effect on changes in serum creatinine, estimated creatinine clearance or the number of patients developing renal impairment, when compared with placebo. Of 18 790 treated hypertensive patients, 41% received an ACE
inhibitor.
D. Pharmacokinetic studies
A single-dose study in 12 healthy subjects found that the pharmacokinetics of benazepril 20 mg and aspirin 325 mg were not affected by concurrent use.
Mechanism
Some, but not all the evidence suggests that prostaglandins may be involved in the hypotensive action of ACE inhibitors, and that aspirin, by inhibiting prostaglandin synthesis, may partially antagonise the effect of ACE inhibitors on blood pressure. This effect appears to depend on the dose of aspirin and may also be dependent on sodium status and plasma renin, and therefore it does not occur in all patients.
The beneficial effects of ACE inhibitors in heart failure and ischaemic heart disease are thought to be due, in part, to the inhibition of the breakdown of kinins, which are important regulators of prostaglandin and nitric oxide synthesis. Such inhibition promotes vasodilatation and afterload reduction.
Aspirin may block these beneficial effects by inhibiting cyclo-oxygenase (COX) and thus prostaglandin synthesis, causing vasoconstriction, decreased cardiac output and worsening heart failure.
Importance and management
Low-dose aspirin (less than or equal to 100 mg daily) does not alter the antihypertensive efficacy of captopril and enalapril. No special precautions would therefore seem to be required with ACE inhibitors and these low doses of aspirin. A high dose of aspirin (2.4 g daily) has been reported to interact in 50% of patients in a single study. Aspirin 300 mg daily has been reported to interact in about 50% of patients in another study, whereas 325 mg daily did not interact in further study. Thus, at present, it appears that if an ACE inhibitor is used with aspirin in doses higher than 300 mg daily, blood pressure should be monitored more closely, and the ACE inhibitor dosage raised if necessary. Intermittent use of aspirin
should be considered as a possible cause of erratic control of blood pressure in patients on ACE inhibitors.
Both ACE inhibitors and aspirin are often taken by patients with coronary artery disease, and ACE inhibitors are used in chronic heart failure, which is often associated with coronary heart disease.
The information about a possible interaction between ACE inhibitors and aspirin in heart failure is conflicting. This may be due to much of the clinical data being obtained from retrospective non-randomised analyses. It may also be a factor of different disease states. For example, an interaction may be less likely to be experienced in patients with heart failure of ischaemic aetiology than those with non-ischaemic causes, because of the added benefits of aspirin in ischaemic heart disease.24 The available data, and its implications, have been extensively reviewed and commented on.Some commentators have advised that, if possible, aspirin should be avoided in patients requiring long-term treatment for heart failure, particularly if heart failure is severe. Others suggest avoiding aspirin in heart failure unless there are clear indications, such as atherosclerosis.
The use of lower doses of aspirin (80 to 100 mg daily rather than greater than or equal to 325 mg daily) in those with heart failure taking ACE inhibitors has also been suggested.24,25,28 US guidelines from 2005 on chronic heart failure33 state that, “Many physicians believe the data justify prescribing aspirin and ACE inhibitors together when there is an indication for use of aspirin,” while recognising that not all physicians agree. The guidelines say that further study is needed. European guidelines state that there is little evidence to support using ACE inhibitors and aspirin together in heart failure. The guidelines say aspirin can be used as prophylaxis after prior myocardial infarction, but that it should be avoided in patients with recurrent hospitalisation for worsening heart failure.
NICE guidelines in the UK make no comment about the combination of ACE inhibitors and aspirin. They say that all patients with heart failure due to left ventricular systolic dysfunction should be considered for treatment with an ACE inhibitor, and that aspirin (75 to 150 mg once daily) should be prescribed for patients with the combination of heart failure and atherosclerotic arterial disease (including coronary heart disease).35 Data from ongoing randomised studies may provide further insight. Until these are available, combined low-dose aspirin and ACE inhibitors may continue to be used where there is a clear indication for both.
An increased risk of deterioration in renal function or acute renal failure appears to occur rarely with the combination of aspirin and ACE inhibitors.
The routine monitoring of renal function, which is advised with ACE inhibitors, should be sufficient to detect any interaction. |
|





 鲁公网安备 37020202001532号
鲁公网安备 37020202001532号 
 学习!加油
学习!加油




 IP卡
IP卡 狗仔卡
狗仔卡
 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 抢沙发
抢沙发 千斤顶
千斤顶 显身卡
显身卡

 楼主
楼主